Complications of Thyroid Surgery
As with any surgery or procedure, there are risks and complications with thyroidectomy.
The risks of surgery are similar between a hemithyroidectomy (half the gland removed) and a total thyroidectomy (the whole gland is removed), but a total adds a few extra. Risks are reduced with surgeons who have more experience.

Complications
- Intra-operative or post-operative bleeding
- Infection
- Damage to the recurrent laryngeal nerve or superior laryngeal nerve
- Hypothyroidism (low thyroid hormone levels)
- Low calcium (hypocalcemia)
- Scar
- Need for re-operation
- Tightness in the neck with motion and swallowing
Intra-operative or post-operative bleeding
Excessive intra-operative bleeding is uncommon and the need for transfusion is rare. This risk is higher for patients getting surgery for hyperthyroidism. Post-operative bleeding is also uncommon but can be dangerous. The hematoma (collection of blood) can cause pressure in the neck and become dangerous.This would necessitate emergently going back to the operating room to stop the bleeding and remove the blood. This is a rare complication. The risks are also higher in people on medications that increase bleeding (warfarin, aspirin, Plavix, etc.), some herbal medicines that increase bleeding (ginkgo, garlic, ginseng), or have specific medical conditions (liver failure, kidney disease, thrombocytopenia, hemophilia, von Willebrand’s disease).
Infection
The risk of infection to the surgical area is very low, and pre-op and post-op antibiotics are not given. Signs of infection are increasing pain, redness, swelling, pus at the incision site, and fever. Treatment will require antibiotics. If there is a collection of pus, surgery may be needed to drain it.Damage to the recurrent laryngeal nerve or superior laryngeal nerve
The recurrent laryngeal nerve controls movement of the vocal cord. Damage causes paralysis of the vocal cord and voice changes described as a breathy hoarseness–like a whisper. People often have to take a breath in the middle of a sentence. Talking takes more effort and the voice is easily fatigued. It can also cause problems with swallowing. The risk is less than 1% with half recovering on their own and half becoming permanent. The actual risk is likely higher with minor trauma to the nerve causing transient hoarseness and vocal fatigue.Minor damage may not be fully apparent and recovers quickly. There are things that can be done to help the voice. A total thyroidectomy puts both nerves at risk (one on each side). Paralysis of both nerves is very rare and dangerous. The vocal cords do not open, breathing can be difficult and may require a tracheostomy tube until a plan can be made regarding treatment of the blockage. Damage to the superior laryngeal nerve causes loss of pitch range.
Hypothyroidism (low thyroid hormone levels)
If only one side of the thyroid is removed (hemithyroidectomy), the side that remains is usually enough to make adequate amounts of thyroid hormone. About 15-20% of people will need to supplement with thyroid hormone pills. Blood levels are checked 4-6 weeks after surgery. People are at a higher risk of hypothyroidism later in life. If the whole gland is removed, there is, of course, a 100% chance of needing to be on thyroid hormone pills after surgery for the rest of your life. Go to hypothyroidism.
Low calcium (hypocalcemia)
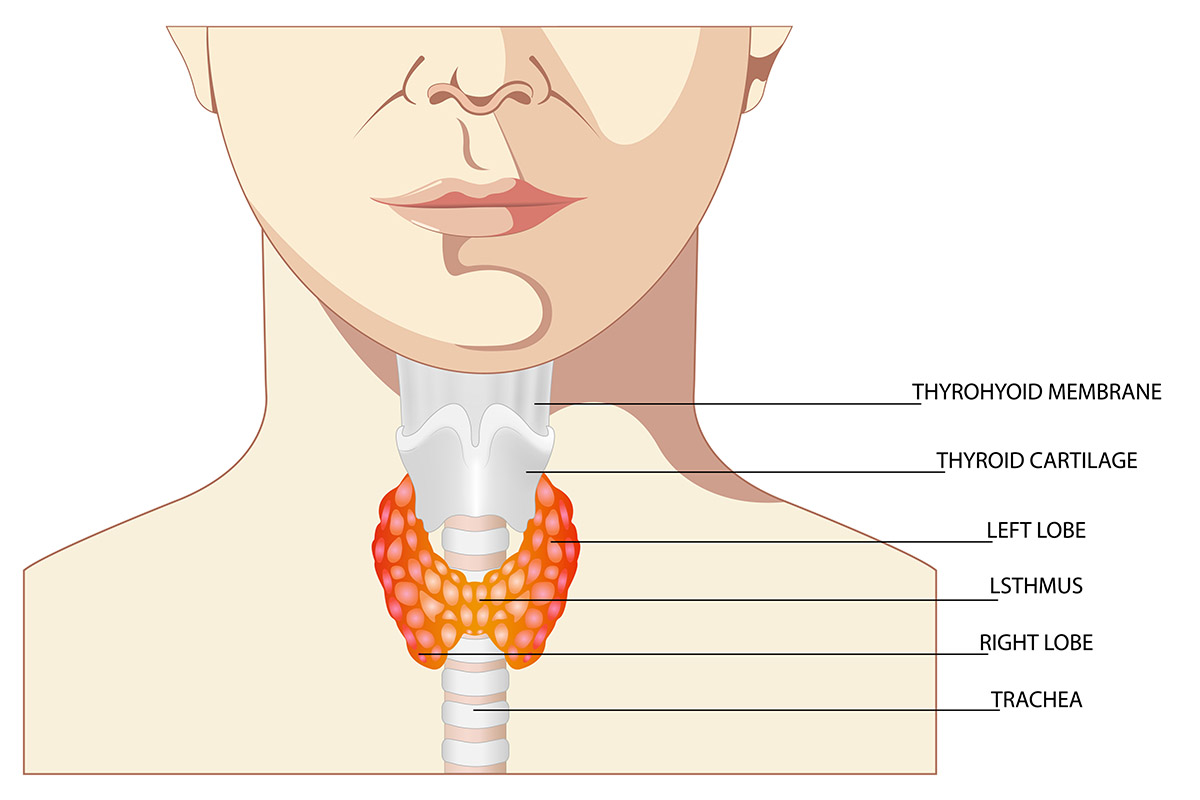
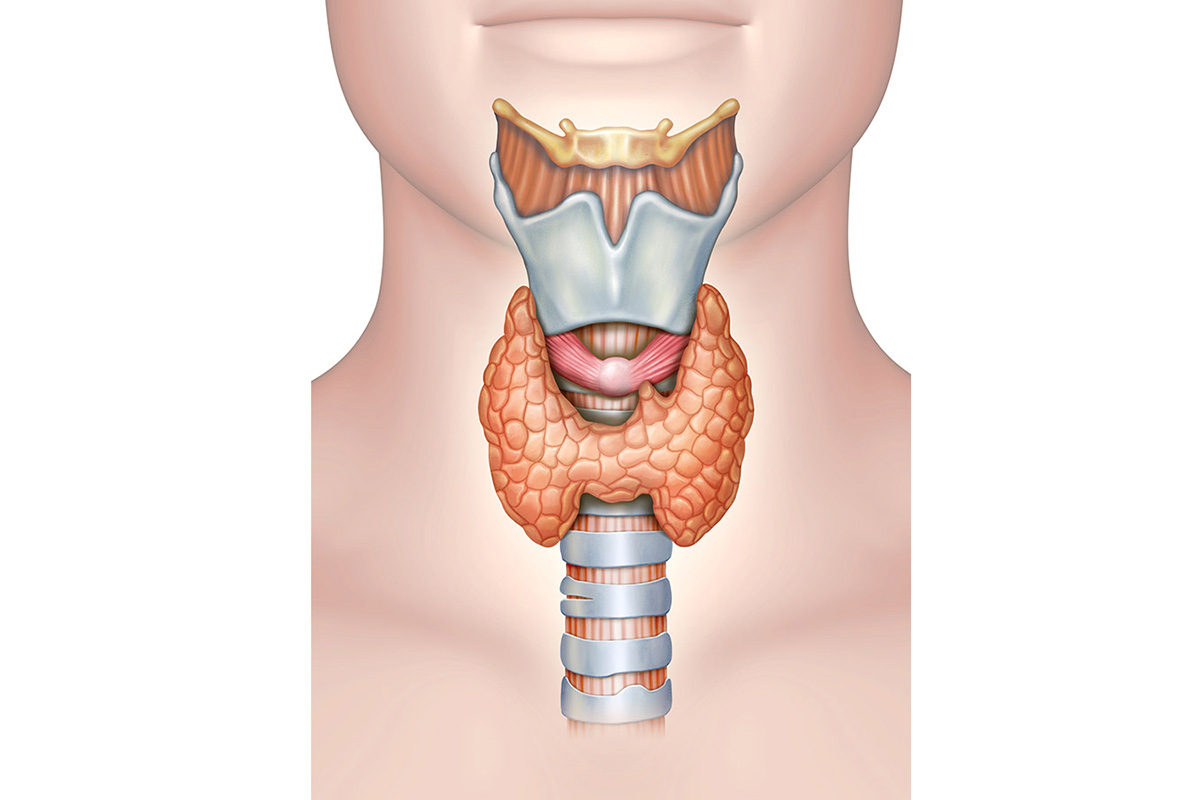
There are 4 tiny glands next to the thyroid called the parathyroid glands. They control the calcium levels in the blood. Manipulation of the parathyroid glands on both sides of the neck (with a total thyroidectomy or completion thyroidectomy) can cause them to stop functioning, and there is a risk of low calcium after surgery. Transient low calcium is common and usually remains asymptomatic. Patients are sent home with oral calcium supplementation and vitamin D to prevent any post-operative symptoms. Prolonged and profound low calcium levels are not common (~2%).As calcium levels drop, symptoms include numbness and tingling in the lips and finger tips. Worse levels lead to muscle cramps and heart arrhythmias that can be dangerous. Spasm of the larynx, called laryngospasm, is possible and can cause dangerous difficulty breathing. If levels get too low then patients need calcium given intravenously and may need to stay in the hospital several days until calcium levels can be stabilized with high doses of oral calcium and vitamin D (calcitriol). If abnormal cramps develop after surgery, then patients will need to be assessed in the emergency department, where they can get stat calcium levels drawn and intravenous treatment.
Scar
Scar is a consequence of any surgery requiring an incision. The placement of the incision for a thyroidectomy helps keep the scar from being very noticeable. Everyone heals differently, so it is hard to predict the final outcome, but most have a very good result.Need for re-operation
Sometimes the problem that causes the need for surgery can recur. If one side of the gland is left, it may develop nodules that need removal. The remaining gland can grow and cause symptoms. This is rare and takes years to develop. Occasionally, a cancer is found when the gland is removed for benign, noncancerous reasons. When that happens, the rest of the gland may need to be removed. If a cancer is the reason for the surgery and it comes back, surgery will have to be done again. Depending on the extent of the cancer, surrounding lymph nodes may also need to be removed.Tightness in the neck with motion and swallowing
Some people feel tightness in the neck or when swallowing during the healing process. This can be helped with neck range of motion exercises and massage.Request an Appointment
Same and next day appointments available